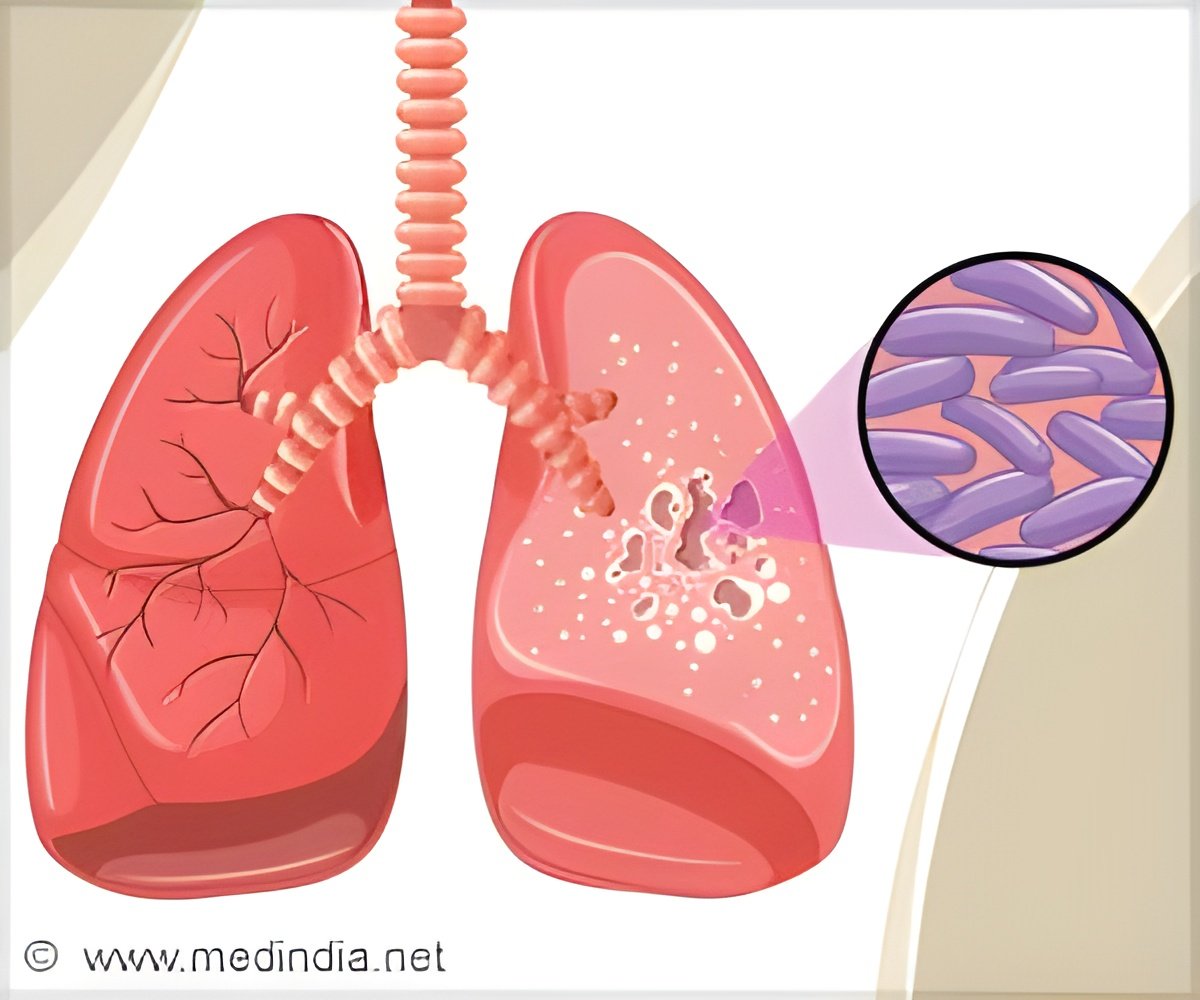

Researchers are exploring innovative immune-enhancing treatments known as host-directed therapies, aiming to harness the body’s immune system to combat tuberculosis, including drug-resistant strains. ()
The reported global number of people newly diagnosed with TB was 7.5 million in 2022, causing an estimated 1.3 million deaths. As estimated 410 000 cases and 160 000 deaths were due to multidrug-resistant TB (MDR-TB).
“Mycobacterium tuberculosis (Mtb) have evolved a remarkable ability to manipulate the human immune response and undermine antimicrobial effector functions in host immune cells,” explains Assoc Professor Brighenti.
“While some new antimicrobial therapies are coming through, treatment with antibiotics remains an intensive and long process even for drug-susceptible forms of the disease. Importantly, mutations conferring antibiotic resistance are intrinsic properties of mycobacteria that effectively develop resistance to old as well as new groups of antibiotics, accentuating the need for adjunct treatments. Thus, new treatments are going to be absolutely vital in the battle against TB.”
Restoring Antimicrobial Functions in Tuberculosis
HDT are designed to target several immune pathways in infected cells to restore or induce antimicrobial functions instead of inhibiting bacterial growth directly. This may involve enhanced production of immune peptides or toxic molecules that contribute to bacterial killing, but it could also include rebalancing of inflammatory responses. Assoc Professor Brighenti will explain how her research collaboration has generated a platform for immune reconstitution in TB, using small molecule compounds including histone deacetylase (HDAC) inhibitors.
“These drugs can regulate transcription of genes in cells such as those in the immune system, and thus enhance the expression of proteins associated with the antibacterial host defense. We have identified several HDAC inhibitors that reduce Mtb growth inside immune cells by some 50-75%, even in the absence of antibiotics,” she explains. “That may not sound so impressive, but these immunomodulatory compounds could work well as a complement to standard therapy and exert additive or synergistic effects together with the antibiotics. This would provide the possibility to reduce the dose and treatment length required with antibiotics to improve patient outcomes.”
In this way, it is conceivable that the effect of existing antibiotics could be guarded by add-on therapies that restore protective immunity and limit excess inflammation and/or immunosuppression in patients with TB. Standard anti-TB treatment involves daily administration of 4-9 antibiotics, but instead of adding yet another antimicrobial drug to the regimen, an immune-enhancing compound could promote clinical recovery of patients with severe forms of TB and poor prognosis, especially MDR-TB.
Advertisement
Assoc Prof Brighenti says “Implementation of immunotherapy as a complement to standard therapy has revolutionized the treatment of cancer, autoimmunity, and asthma/allergy. Similarly, our research on immune enhancement as a complement to antibiotics may become a game-changing treatment option for patients with TB that has the potential to impact clinical management and prevent spread of TB infections and drug resistance in this pivotal moment in our history when antimicrobial resistance constitutes a serious threat to human health.”
She adds: “Short-term, approved and already available ‘off-the-shelf’ therapeutics would represent an initial logical step to implement HDTs of patients with TB. This could include for example, HDTs based on glucocorticoid treatment or cytokine neutralization (eg. anti-IL-6, anti-1β) to reduce inflammation, while metformin, or non-steroidal anti-inflammatory drugs may also promote or rewire the immune response.
Advertisement
“Long-term, more precise immunomodulatory interventions in TB such as local administration of specific HDAC inhibitors, can be tested in clinical trials with the aim to customize therapy for patients with MDR-TB. Today, several HDAC inhibitors are FDA-approved for different diseases – for example, Vorinostat, Belinostat, and Panobinostat for different cancers, Phenylbutyrate for urea cycle disorders and Givinostat for Duchenne muscular dystrophy, while the ones we have found to be most effective to reduce intracellular M. tuberculosis growth needs to be first tested in pre-clinical models for toxicity and efficacy before progressing to clinical trials.”
Importantly, like many other diseases, TB can be divided into different sub-groups and using a one-fits-all approach to treatment is not necessarily best. Tailored treatments that are optimized to individual patient needs, so called personalized medicine, will also be part of the future for TB management.
Reference:
- Experts develop immune-enhancing therapies to target tuberculosis – (https://www.eccmid.org/)
Source-Eurekalert